Clinical Case Detail
Return to Clinical Case List
CPC Case #3
Provided By
Russell E. Christensen DDS - 2010-05-12
Clinical History
The patient is a female, approximately 40 years of age
She complains of bleeding, pus and pain from a palatal lesion for about 10 days.
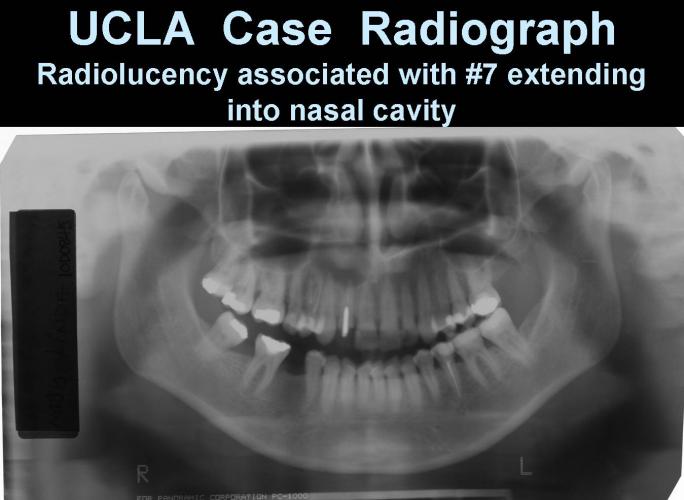
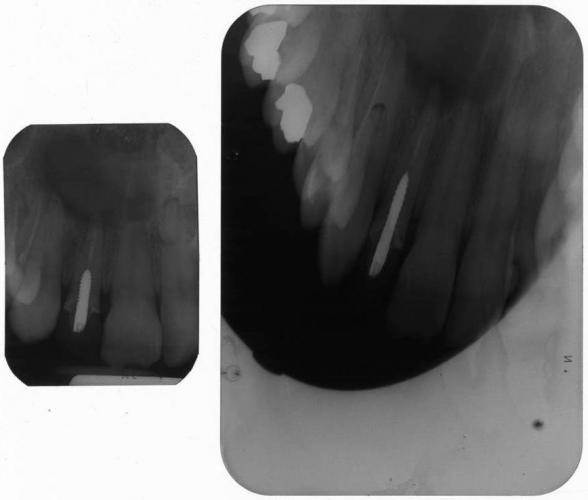
There is a large radiolucency associated with the apex of # 7 (endodontic treatment of # 7 performed outside USA)

Differential Diagnosis
* Hereditary/developmental
* Infectious/Inflammatory
- From RCT
- Fungal
* Physical injury/foreign material
- From RCT
* Metabolic/Medications
* Neoplastic/Reactive Tumors
* Allergic/Autoimmune
- Wegener's Granulomatosis
Plan
* Biopsy
* Imaging
- Chest film
* C-ANCA
* Urinalysis
Preliminary lab results
* Urinalysis: WNL
* Chest film: WNL
* C-ANCA: negative
Revised Plan
* Obtain history from non-relative
- Positive for cocaine use in past
* Extract lateral incisor and microscopically examine tissue
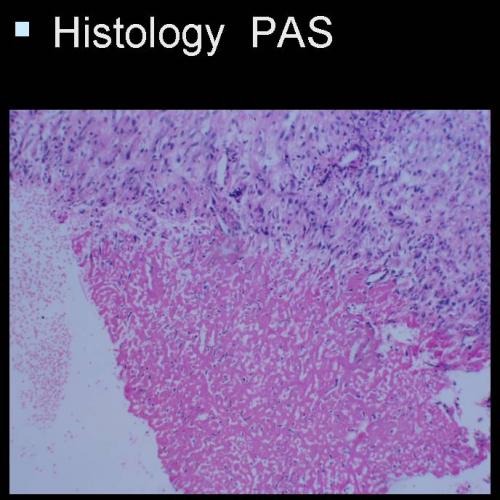
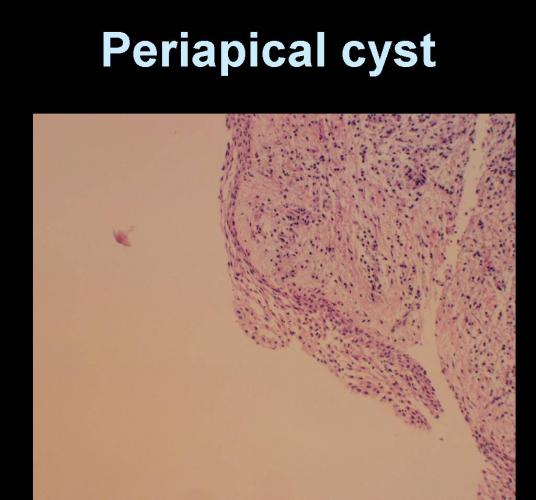
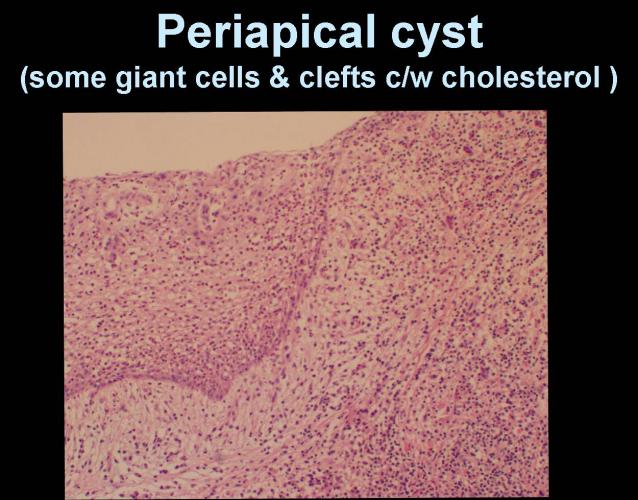
Diagnosis
#1 RTC-related foreign material (unknown)
#2 palatal perforation from cocaine insufflation
Clinical Features
Surgical findings at time of extraction
* Palatal defect healed except for barely detectable pinhole fistula
* Periapical lesion with thick capsule and no detectable communication with palatal defect
Radiographic Findings
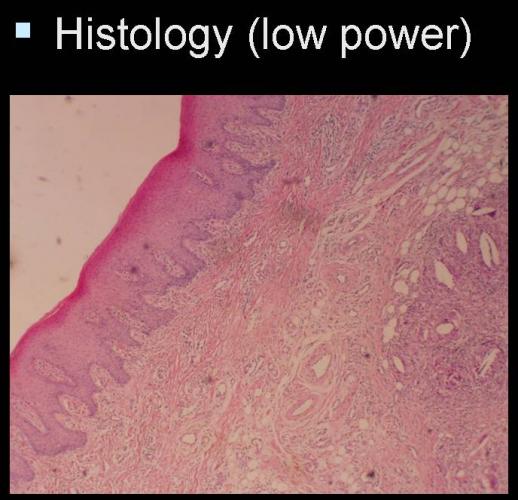
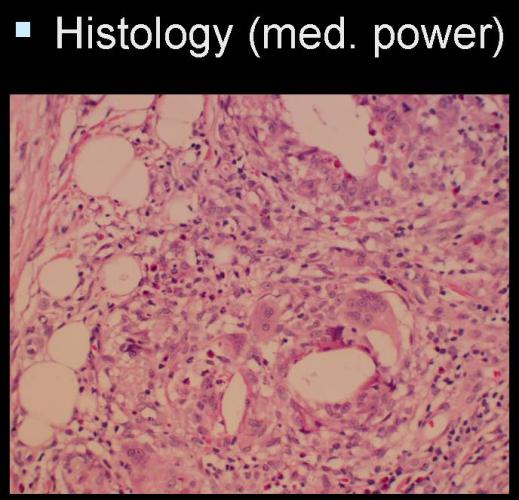
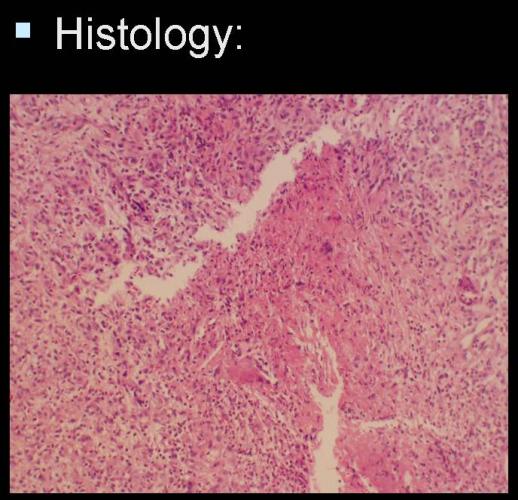
Discussion
* Seyer BA, Grist W, Muller S: Aggressive destruction midfacial lesion from cocaine abuse. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 94:465-470
* Local vasoconstrictive effects
* Cut with talc, borax, plaster of paris, lactose, amphetamines, mannitol
* Inflammation & ischemic necrosis as early as 3 weeks after "binge"